ELIMINATE MATERNAL MALNUTRITION
YOUNG WOMEN HOLD THE KEY TO NUTRITION ADVANCES
Poor nutrition causes a massive burden of death and disability in the world, with nutritional deficiencies responsible for 252,000 deaths and obesity a risk factor in five million deaths, according to the Global Burden of Disease (GBD). One in three people on the planet is malnourished, and every country is now struggling with malnutrition in some form, ranging from underweight to obesity.
The costs of this burden of malnutrition are enormous, impeding not only population health improvements but also economic growth and development. Failing to act on malnutrition is costing low-, middle-, and high-income countries billions of dollars in healthcare costs and lost worker productivity every year. On the other side, investing in nutrition can deliver big benefits. For example, every $US1 invested in reducing child malnutrition can save up to $US166, according to the Copenhagen Consensus.
Malnutrition in all of its forms – underweight, obesity, and micronutrient deficiencies – disproportionately impacts women. More women than men are underweight and obese, according to the NCD Risk Factor Collaboration and many more women suffer from iron-deficiency anemia than men. A massive 30% of all women and 37% of pregnant women are anemic, according to the World Health Organization (WHO). As a result, deaths from malnutrition are concentrated among women. Nutritional deficiencies kill more women than men, and high body mass index (BMI) contributes to more deaths among women than men, according to the GBD.
Malnutrition among women aged 15 to 49 is particularly concerning because of its impact on both women’s and children’s health, as well as on labor force and on educational performance.
Women who are malnourished (underweight or obese, and/or micronutrient deficient) are more likely to experience maternal death and birth complications – including babies born preterm, with low birth weight, and/or with congenital defects. If these babies survive, they are at increased risk of malnutrition. In 2022, there were an estimated 149 million stunted children, 45 million wasted children, and 23 million born with low birth weight, according to WHO.
As the major providers of nutritious food for their children and families, women of reproductive age also exert a profound influence on the nutritional status of future generations, especially in the vast majority of countries where women are wholly responsible for family food preparation.
In recognition of women’s leadership role in family nutrition, efforts to improve mothers’ agency to provide nutritious foods and to create a healthy home environment, in a way that doesn’t impede female labor force participation, should be at the center of nutrition policies and programs. In this context, the ability of women to breastfeed and to cook meals that do not contribute to the dangerously high levels of household air pollution should be part of a maternal nutrition agenda.
There needs to be wider recognition that reducing current levels of malnutrition, and arresting its intergenerational cycle, depends on the level of support provided to improve the daily lives of women of reproductive age.
MALNOURISHED WOMEN ARE CONCENTRATED IN SPECIFIC COUNTRIES
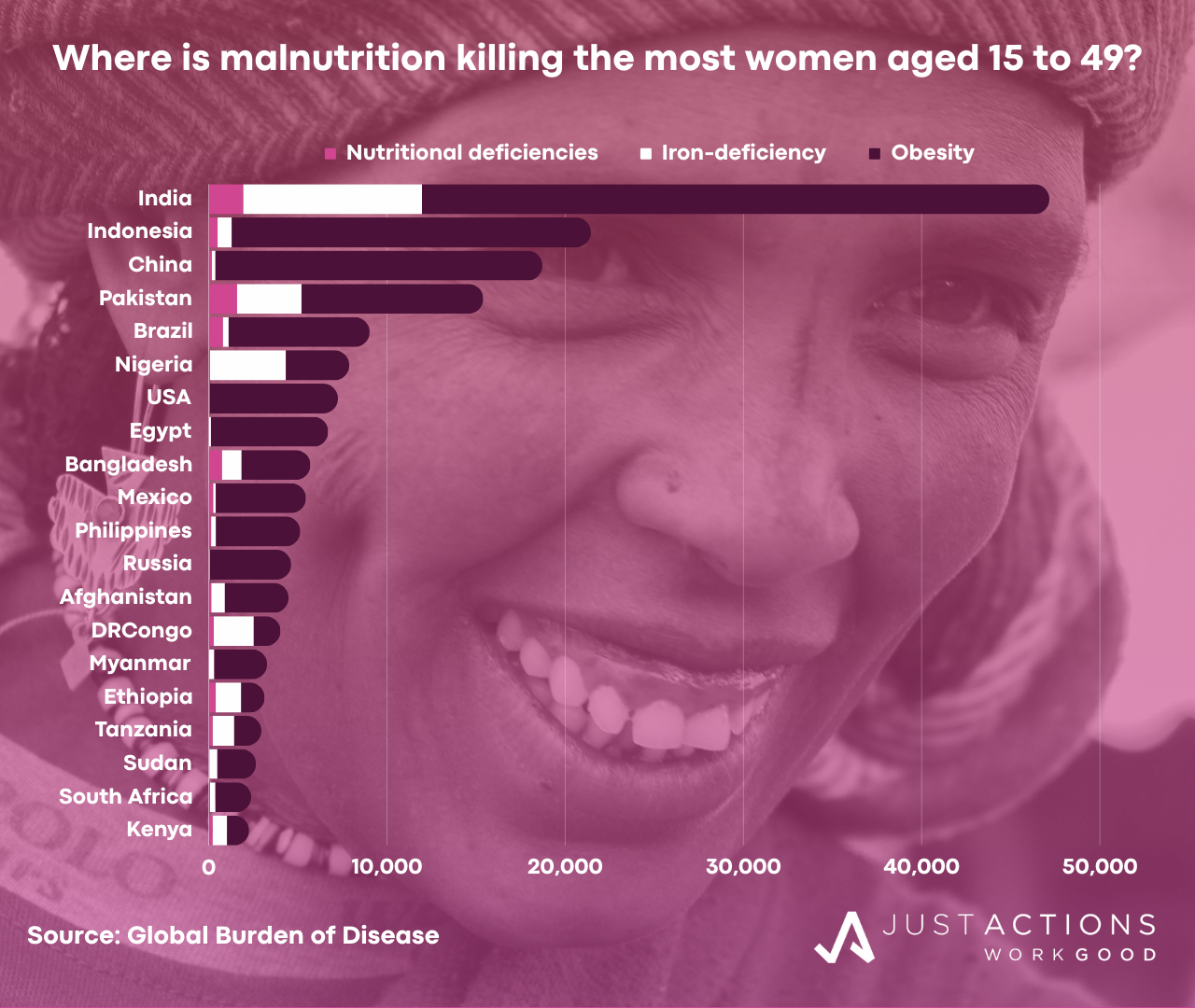
Malnutrition among women of reproductive age is concentrated in 20 countries. More than half of the annual (2019) 10,500 deaths from nutritional deficiencies among women aged 15 to 49 occur in just five countries including India, Pakistan, Bangladesh, Brazil, and Indonesia. Similarly more than half of the 204,000 obesity-related deaths among young women occur in a five countries including India, Indonesia, China, Pakistan, and Brazil.
India, Pakistan, Brazil, and Indonesia appear on both lists as they are part of a growing number of middle-income countries struggling with “double burdens” of malnutrition – high rates of undernutrition and obesity.
For example, in India an estimated 1,900 young women aged 15 to 49 die from nutritional deficiencies each year, while 35,000 die from obesity-related causes. In Pakistan, an estimated 1,600 young women die from undernutrition, while 10,000 die from obesity-related causes. In Brazil, 7,900 women die from obesity compared to 800 women from nutritional deficiencies. And in Indonesia, an estimated 500 young women die from undernutrition, while 20,000 die from obesity-related causes. As deaths from undernutrition fall in most countries, deaths from obesity are rising, often precipitously.
In addition to the risks of underweight and obesity, micronutrient deficiencies cause a large burden of disability, especially anemia, and related deaths. For example, in India, one-half of all women aged 15 to 49 (188 million) are anemic and almost half of all women enter pregnancy underweight, according to research by Diane Coffey. Many western and central African countries are also struggling with anemia prevalence rates of above 50%.
Iron deficiency is a risk factor in 42,000 deaths among women aged 15 to 49, with most deaths in India, Nigeria, Pakistan, the Democratic Republic of Congo, and Ethiopia. In many of these countries, anemia-related deaths among young women are not falling, including in India, Nigeria, Pakistan, and Ethiopia, according to the GBD.
As a result, no country is on track to meet the World Health Assembly target of halving the number of women of reproductive age who are anemic by 2025. In fact, of all the nutrition targets, reducing anemia is the most off-track, according to the Global Nutrition Report.
REDUCING MATERNAL MALNUTRITION: A NEW DEVELOPMENT PRIORITY
As the burden of nutrition-related death and disability is concentrated among women, and in recognition of the critical role women play in determining the nutritional status of populations, national nutrition strategies should focus on improving the nutritional status of women of reproductive age and on strengthening their capacity to provide nutritious diets for themselves, their children and their extended families.
Accordingly, countries should set targets for halving underweight and anemia among women 15 to 49 years by 2025 and for eliminating both by 2030. In addition, governments should set new targets of halving obesity rates among women aged 15 to 49 by 2030.
To achieve these goals, all nutrition stakeholders should work together to simultaneously increase the supply of foods and supplements designed to meet the special nutritional needs of women, especially during pregnancy, and encourage their use by educating women, by providing cash transfers conditional on their use, by offering nutritious foods and supplements as incentives for healthy behaviors (e.g., childhood vaccination, prenatal care visits), and by making foods and supplements available at the places women frequent daily (e.g., schools, workplaces and shops). Financial incentives conditional on specific behaviors should also be applied to reduce obesity rates.
Urgent action on the consumption of iron-folic acid supplements and iron-fortified staple foods is required, alongside protein-energy foods and supplements especially for adolescent girls and pregnant women in the countries where iron-deficiency prevalence and related deaths are highest.
Women should be encouraged to use these products through a mix of education and cash and non-cash incentives, which the World Bank concludes can improve nutrition, especially when delivered directly to women.
Incentives can include cash directly to mothers or rewards such as mobile phone minutes, energy subsidies, access to job information, educational supplies for children, or other rewards valued by specific populations. Another model is to link food rewards to compliance with other health and related programs.
For example, when Indian women were offered a food reward (lentils) upon completion of their child’s vaccination schedule, full vaccine coverage went up substantially and family nutrition improved, according to the Poverty Action Lab.
Given the gender dynamics within families, care needs to be taken to ensure that special foods meant for women actually reach them, via special labeling, custom formulations that cannot be taken by children, and/or consumption on site at schools or workplaces. Programs that incentivize fathers to prioritize the nutritional status of their wives and daughters should also be explored.
For example, an analysis by Rohini Pande and Seema Jayachandran suggests that the lower nutritional status of women in India starts very early in life. Their study revealed that firstborn children in India are actually taller than firstborn African children and that stunting emerges within Indian families only after the arrival of the first son. This suggests that India will never end child malnutrition without broader shifts in parental attitudes towards daughters.
Incentives should also be provided to enable women to breastfeed in hospital, at home and at work and to transition to cooking methods that do not create the high levels of indoor air pollution that are contributing to a massive burden of death and disability. Early and exclusive breastfeeding can protect newborns from infection as well as contribute to their growth and most of the countries that have reduced child deaths by two-thirds since 1990 have exclusive breastfeeding rates above 50%.
The University of Sheffield has conducted trials to test whether cash payments for breastfeeding can lift rates well above the current low levels in the UK and there needs to be much more experimentation with new approaches to enable breastfeeding (e.g., low-cost breast pumps, paid leave, human milk banks, employer rewards for breastfeeding supportive workplaces etc.). Incentives are also being tested to encourage the use of clean energy for cooking and heating.
It is important that nutritional foods and supplements are accessible to women in the course of their daily lives and do not add any further inconvenience. Recent work by GAIN and Alive & Thrive to encourage large employers of young women in Bangladesh and Viet Nam to educate women about nutrition and to provide nutritious foods and breastfeeding support at work is one example of how to reach women without asking them to incur additional costs.
Another way is to deliver foods and supplements alongside other services (e.g., polio campaigns, prenatal visits, and medicine distribution during disease eradication campaigns). For example, the Clinton Health Access Initiative, the Children’s Investment Fund Foundation, Nutriset, the Government of Nigeria, and UNICEF recently collaborated on a campaign in Nigeria where children received nutritional supplements alongside their malaria medicines, protecting them against the double scourge of malaria and malnutrition at a particularly vulnerable time of the year.
All of these investments in improving the nutritional status of women of reproductive age will bear fruit for children’s nutritional status. 70% of the recent reduction in childhood stunting in Bangladesh is due to advances in education, incomes, sanitation and contraception, most of it among women aged 15 to 49 years, according to the Global Nutrition Report.
SUPPORT THE REAL CHAMPIONS OF NUTRITION: MOTHERS
Achieving the Sustainable Development Goal to “end” hunger and all forms of malnutrition by 2030, with its special focus on reductions in child stunting and wasting and meeting the nutritional needs of adolescent girls, and pregnant and lactating women, will depend upon how well women of reproductive age can improve their own nutritional status and their children’s.
The goal to reduce early deaths from non-communicable diseases by one-third will also rely heavily on reducing rates of obesity among women, which often rise during the reproductive years. The United Nations (UN), its agencies, and partners should affirm that prioritizing the nutritional needs of women of reproductive age will accelerate the achievement of all nutrition goals.
The UN should encourage development partners with a stake in meeting these goals to increase investments in high-impact interventions with a proven track record of improving women’s own nutritional status and their capacity to improve family nutrition, with priority given to the largest populations of malnourished women.
Full engagement of the private sector is required to achieve these goals as food is a private market transaction in all but the most fragile of humanitarian settings. The makers, distributors, advertisers, and sellers of the vast majority of foods that people consume are profit-seeking individuals and companies. Not only do companies provide food, but they are also in steady dialogue with consumers through their marketing channels which are becoming ever more sophisticated with rapid income growth and urbanization occurring everywhere alongside rising consumption of processed foods.
The degree to which those committed to achieving the new global nutrition goals can influence the exchange of information and food between food and beverage companies and populations of women 15 to 49 years will largely determine their achievement.
The UN should also lead the charge in a data revolution that would fill the unacceptable gaps in our knowledge of the nutritional status of women of reproductive age at national and sub-national levels.
The world urgently needs information on the nutritional status of women, down to state and district levels, especially in the countries with the largest numbers of nutrition-related deaths. For example, it should be as simple as visiting a website to find out the numbers of women aged 15 to 24 in the districts of Uttar Pradesh, India who are underweight, or the numbers of pregnant women who are obese in Sindh Province, Pakistan, or the areas within Kano State, Nigeria with the highest rates of female anemia.
A final note. There is often talk of the need for nutrition champions among government and development leaders. But the real champions of nutrition are the hundreds of millions of disempowered women who are responsible for feeding future generations under the most challenging of conditions.
It is often these women, mostly mothers, who shoulder the burden of farming, shopping, cooking, and feeding families when they themselves are struggling with poor nutrition, low levels of education, and severe restrictions in their ability to earn an income and to make financial decisions. Enabling these women to take the actions necessary to safeguard their own nutrition and that of their children can unlock the next wave of nutrition advances.
Updated January 2024